
Use interactive elements to keep the learner engaged
Challenge #1: The MSL team has not worked with epidemiologists in the past.
Challenge #2: Building a foundational knowledge base on a subject is challenging (and sometimes perceived as ‘boring’)
Challenge #3: The value of spending time learning about basic information is not always communicated
MSLs require prior knowledge to discuss science with physicians
A Medical Science Liaison (MSL) has an appointment with a clinical expert in infectious disease to discuss information published by the World Health Organization (WHO) about ‘Pandemic Preparedness and Response.’ The meeting is to better understand physicians’ interpretations of viruses with pandemic potential.
The position paper presumes prior knowledge of epidemiology. The MSL’s scientific experience was supplemented with further training provided by their employer. The Medical Affairs department invested in the creation of multiple resources regarding therapeutic areas of interest. After the initial onboarding phase of training, the MSL was able to create their own personalized curriculum from a library of courses. The MSL’s continuous education has prepared them to engage in scientific exchange at a deeper level with this well-respected health care provider (HCP).
Onboarding is often only product focused
Medical Affairs teams are often composed of employees with advanced scientific and medical credentials. However, as with all new employees regardless of education level, there are always knowledge gaps. In the scenario above, the company found it necessary to provide additional scientific training despite the scientific expertise of the newly hired MSL.
Part of an MSL’s daily role is the discussion of general disease states topics with HCPs. These discussions can be especially enjoyable for scientific exchange because they are not product specific and thus, the HCP does not feel as if the MSL is “selling” something. However, medical affairs onboarding often focuses on product-specific information to the detriment of general foundational knowledge. How does the employer balance the need for immediate, specific knowledge with longer-horizon, generalized information?
Consider Longer Term Data Needs
The employer conducted a curriculum review that included an assessment of topics to make available to the team after initial onboarding. A menu of advanced topics was built out over time. A strong learning experience was crafted by creating a website façade that linked the training to the corporate LMS in a seamless experience.
To the employees, it was like a Netflix experience – every few months a new range of ‘shows’ became available. The Learning & Development team re-prioritized new content based on MSL needs in the field and requests from the team. A comprehensive communication plan ensured that employees were aware of the offerings and how to access them – 24/7.
Engage the learner during training –
even when it is asynchronous
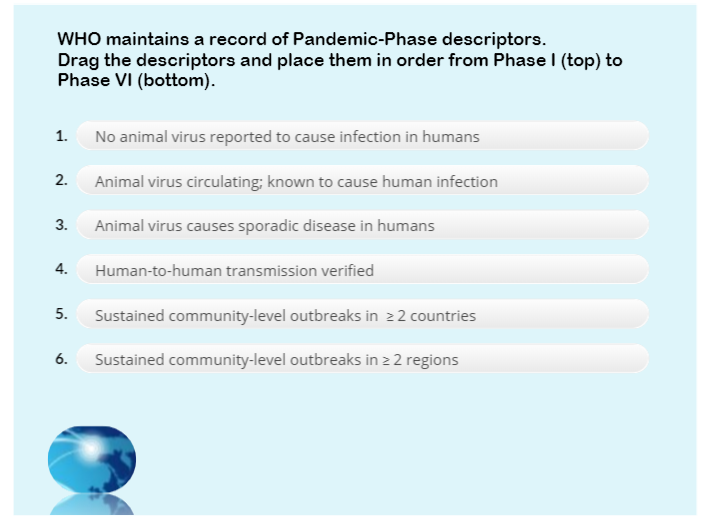
In the training example shown here, the learner has a non-graded opportunity to organize the sequence of events that make up the phases of
A drag-and-drop interaction is a great option for organizing information in a sequence.
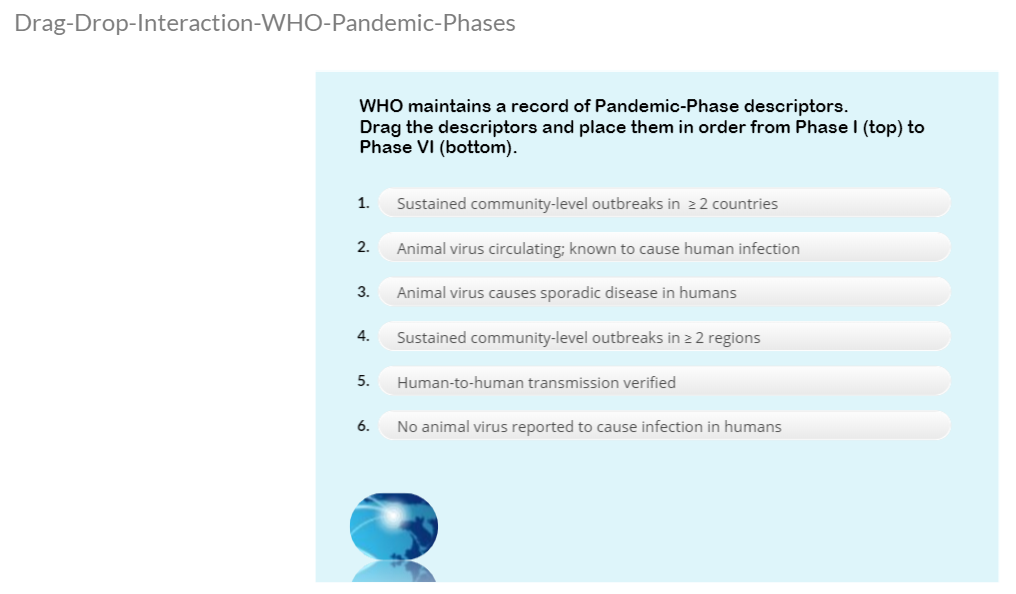
The learner drags each item to create the correct sequence of phases, from first to last, as shown to the right.
Each time the scene is viewed, the six items randomly sort.
Is this the correct sequence?
The learner submits the challenge.
Wrong!
Feedback is provided if the learner provides the wrong sequence.
The learner then has an opportunity to try again…
…and receives positive feedback when the question is answered correctly.
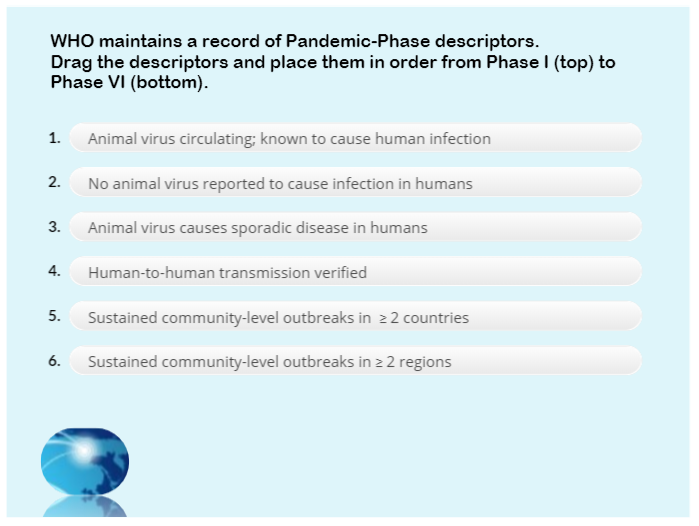
Here is the key for the drag-and-drop (from the earliest to the final event):
- No animal virus reported to cause infection in humans
- Identified reassortant animal virus circulating and known to cause human infection
Animal virus causes sporadic disease in humans- Human-to-human transmission verified
- Sustained community-level outbreaks in at least 2 countries in one region
- Sustained community-level outbreaks in at least 2 regions – 3 countries total
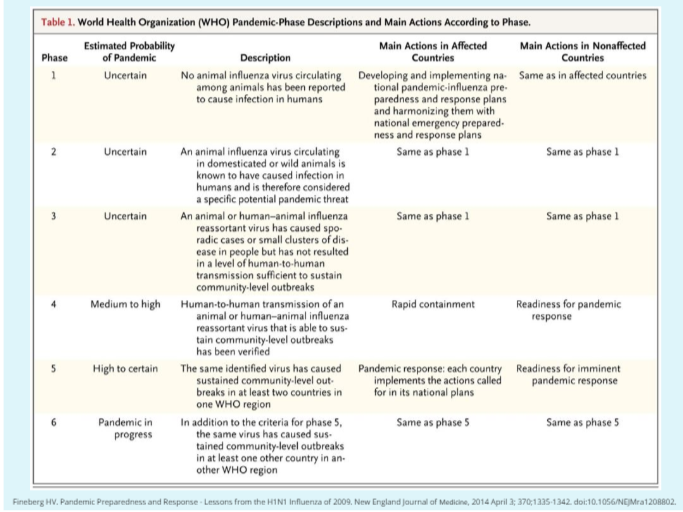
This section of information is summarized by showing the table from the publication:
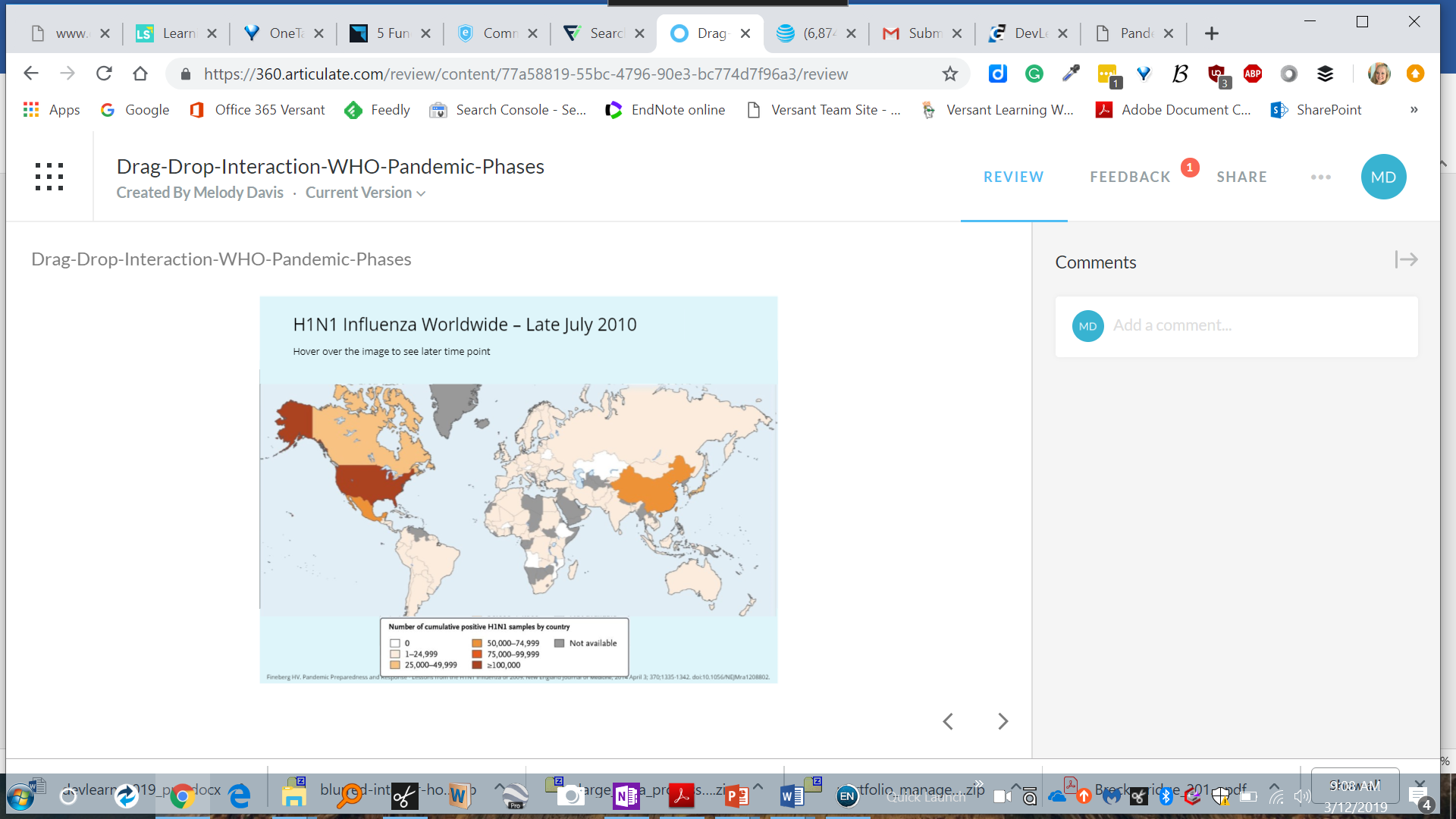
Lastly, the learner can view a map demonstrating the global level of H1N1 influenza cases in April 2009…
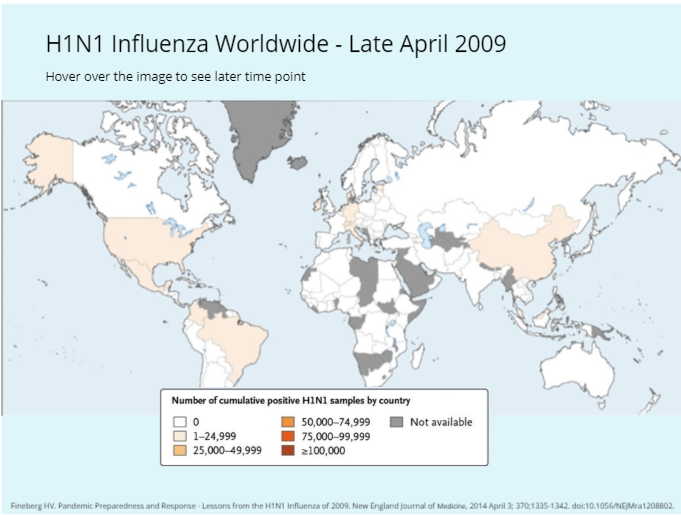
…and by hovering over the map, reveal the number of cases in July 2010.
Let's chat!
If Versant Learning Solutions can assist your team to develop course material, or just discuss possibilities, we would be happy to help!
Reference:
https://www.nejm.org/doi/full/10.1056/NEJMra1208802?query=featured_infectious-disease
Fineberg HV. Pandemic Preparedness and Response – Lessons from the H1N1 Influenza of 2009. New England Journal of Medicine, 2014 April 3; 370;1335-1342. Doi:10.1056/NEJMra1208802.